Teeth come in sets!
It is very important to replace missing teeth in a timely fashion. Obviously, most of our patients want and insist on replacement of missing front teeth as soon as possible, and we accommodate these wishes. Unfortunately, it is tempting to defer less noticeable missing back teeth, and when these fall into the “someday/maybe” category of urgency, long term oral health effects of their non-replacement sometimes catch up to us.
The main reason we need to replace missing teeth as soon as possible is that teeth move. We know this intuitively because we’ve all seen some of the dramatic changes braces and clear aligner treatments can produce, and this is possible only because teeth are able to move from crooked to straighter positions.
The difference between teeth movement that results from missing teeth and the movements produced by braces is that orthodontic movement is intentional and guided, while missing spans, left long term, allow unwanted movement of teeth, as teeth shift positions and angulations in an attempt to come into contact with another tooth.
X-rays in figure 1 show an example of unwanted movement. Patient lost all of his upper molars on the left side when he was younger, as well as a molar on his lower left side.
We can see that the lower molars have leaned sideways until the molar came into contact with the premolar in front of the span, and the molars have erupted upwards in an effort to come into contact with the upper molars that aren’t there. Unlike rabbits and hamsters, our roots don’t keep growing, so eruption of teeth upward has resulted the molars being less securely embedded in the jaw, and loosening has resulted.
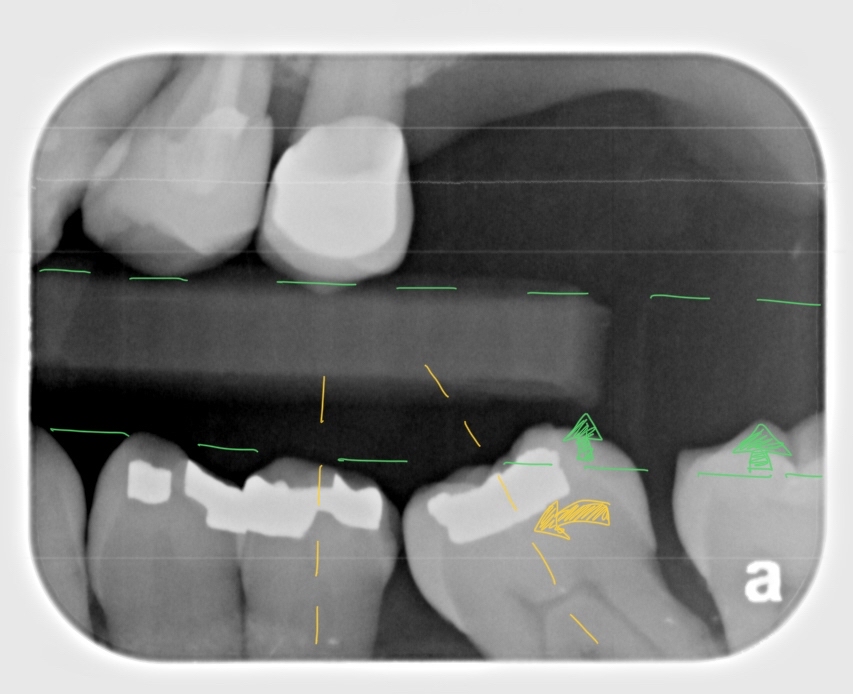
Unwanted Drifting of Teeth (Fig1)
In addition, we can see that while the molar has successfully tilted sideways to come into contact with the premolar, it now sits diagnoally, and large, unnatural food trapping spaces have resulted. We can also see that the remaining lower molar was in traumatic contact with the upper molars (before he lost the upper molars), causing abnormal wear on the molars. This likely contributed to the loss of his upper molars.
Unfortunately too often, patients decide to do something about their chronic food trapping and uncomfortable bite issues too late, after hygiene and traumatic bite issues have caused additional dental illnesses, like localized advanced bone loss, caries and tooth fracture, necessitating more treatment, cost and time.
There are many reason teeth can be lost – severe cavities, bone loss, infection & trauma to name a few. While we can’t really do anything about the past, we have every agency over today and tomorrow to take steps to prevent that lost tooth from triggering additional problems.
We heavily emphasize prevention and early treatment as a practice philisophy, but since replacement of missing teeth is one of the last steps in a complete treatment plan, it often ends up being put off for too long, due to limitations placed by patient’s finances, time constraints, insurance benefits, etc.
3 Ways to Replace Missing Teeth
There are tyically 3 ways within dentistry to replace missing teeth, with each type of prosthetic replacement being appropriate or inappropriate for different patients, depending on the situation, patient’s expectations and requirements regarding esthetics, function and comfort.
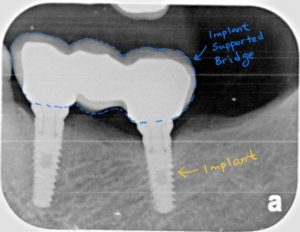
IMPLANTS
Implants are artificial roots, often made of biocompatible titanium, much like artificial joints, which fuse to the bone during their healing process. .
Since what is missing is the tooth and the roots that used to support them, crowns supported by implants represent the most complete replacement of missing structures available. Replacement of missing teeth with implant supported crowns are also the most tooth-like option in terms of hygiene (being able to floss without use of any special tools) and chewing function. Implants also exercise the jaw bone around themselves, preventing atrophy and bone loss that naturally occurs when a tooth is lost.
Implants are also versatile, and can be used to support bridges and hardware to help retain or support dentures.
Some of the disadvantages of implant treament are that they often, but not always, require longer healing times, are more costly than other options, and have requirements regarding quantity and quality of jaw bone they will be placed in, which the other two options do not. There is also an age-limit, where a growing patient is not able to have implants until their growth is completed – usually ~18 years of age for girls, ~20~21 years for boys.
BRIDGES
Bridges are a series of crowns, often with a prosthetic tooth that floats above the missing tooth span, supported by crowns on the adjacent teeth in front of and in the back of the missing tooth.
Bridges, like implants, are fixed prostheses – meaning they are not removable by the patient, and often can be very esthetic. Tooth-supported bridges often also require less healing time than implants (as nothing is placed in the bone) and thus are perceived as quicker treatments by many patients.
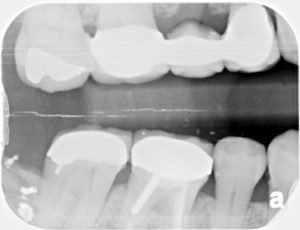
For example, a root fracture caused the premolar in this patient to be extracted.

After extraction, we were able to fabricate a bridge in 2 weeks. The permanent bridge was placed with a temporary cement, in anticipation of additional bone loss in the extraction socket. The bridge will be removed, if necessary, in about 6 months, and have porcelain added to close the gap between the bottom of the prosthetic tooth and the gums.
Bridges, while a popular tooth-replacement choice, have some limitations.
First, they require some sacrifice of adjacent tooth structure, and these teeth in front of, and in the back of the missing tooth, need to be sufficiently strong and healthy to support the additional bite force of the prosthetic tooth. All crowns require reduction of tooth structure to gain space for the thickness of the crown, but bridges place an additional requirement that all teeth supporting the bridge must be parallel or line up, regardless of whether they actually. This sometimes requires aggressive reduction of adjacent tooth structures to fulfill the requirements of the bridge, resulting in the need for root canal treatment in addition to the bridge.
Secondly, bridges do not prevent bone atrophy below the prosthetic replacement tooth, and after some years, a space opens up between the hanging prosthetic tooth and the gum/bone.
Thirdly, bridges, since they are multiple units of crowns splinted together, can not be flossed without use of floss threaders. While this additional step isn’t too onerous, because it is an additional step, the teeth involved in the bridge often get flossed less, and over time, caries in any 1 tooth supporting the bridge requires replacement of the entire bridge.
DENTURES
There are many types of dentures of many different material types, and whether they replace all the teeth in an arch or have a few teeth remaining to hold on to.
Dentures are commonly removable, and must be removed frequently for hygiene, and to sleep.
While less preferred by most patients, dentures have the advantage of being (1) the least invasive tooth replacement option and (2) easy to maintain in terms of hygiene.

Since two dentures (upper and lower) can replace all of the missing teeth in a person’s mouth, they are often the most economical choice.
Dentures are also the most modifyable tooth replacement choice, and are good transitional or temporary prostheses. For example, if someone fractures several front teeth in a way we can not save them in a car accident, an acrylic partial denture (called stay plate) can be fabricated before extraction of the fractured front teeth, and placed immediately the extractions, meaning patient does not have to walk around with no front teeth. The stayplate can then serve as a temporary prostheses, while we wait for healing to occur.
KEEPING REPLACEMENT OPTIONS OPEN
When an extraction is done in our practice, an additional procedure called Socket Preservation Grafting is almost always recommended in conjunction. Socket Preservation Grafting preserves the bone that used to hold on to the extracted tooth root and minimizes bone atrophy that naturally occurs, to preserve the width and height of the jaw bone in the missing tooth area.
This is important because it allows for the optimum placement of an implant of sufficient length and diameter that will withstand the bite forces that will be put on it, or allow for a more esthetic bridge with less food trapping by minimizing bone loss under the prosthetic tooth, or create a rounder, less sharp contour of bone that will comfortably support a denture.
The Right Choice for You
I briefly went over some of the tooth replacement options and some of the clinical considerations involved with each, but in reality, there is no single “best” option for all patients.
Determination of the most appropriate choice of prosthesis depends on a multitude of factors, which need to be evaluated in person, with radiographs, along with your general health history. Experience has taught me that as important as replacing missing teeth is, there are also “outside-the-office” patient considerations that affect when and how we will end up treating these conditions. These can include cost, insurance coverage, upcoming weddings, graduations and other special occasions, a major car repair, an upcoming tuition bill or whatever else is important to the patient.
I think it’s important to realize that to design the best treatment plan that fits your needs, we need to know what’s important to you, regardless of what it is. Open and honest communication, we find, leads to the best outcomes because it produces the most feasible solutions. With the treatment modalities, technology, experience and specialist/laboratory relationships at our disposal, I think you’ll be surprised at the kinds of solutions that fit your dental and life needs that can be designed, whether that involves doing some minimal things to keep you feeling and looking better for now, or definitively treating some long standing issues that have been bothering you for years. .